Whether to remove moles or not is a personal matter for everyone. This depends on many reasons: aesthetic and medical. What to do if a mole grows after removal? Is this hazardous to health? People who have encountered similar troubles often ask such questions. In any case, if the nevus recurs, you should consult a dermatologist who will help you deal with this problem.
The growth of a new mole at the site of a removed one is not a rare phenomenon that can be avoided with proper postoperative care.
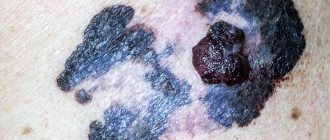
What does relapse of melanoma look like?
Recurrent neoplasm differs from primary melanoma not so much in appearance as in the total volume of the lesion. Often secondary formations are very similar to the previously removed maternal one, only there are many more of them, they can be larger or smaller.
In domestic oncology, there are four types of melanoma relapses according to Wagner’s classification:
- local - the tumor is located exactly in the area of the primary operation;
- transit metastases or satellites - next to the scar, but no closer than 2 centimeters, can be localized not only in the skin, but also in the subcutaneous tissue;
- regional metastases - damage by a malignant process to the lymph nodes near the operation area;
- distant metastases - secondary melanoma tumors in other organs and tissues.
The patient can have relapses of any type and in any set, all at once, which is not surprising for such an aggressive tumor.
Causes of melanoma recurrence
It is assumed that the source of development of a recurrent or metastatic tumor is a malignant cell preserved in a blood or lymphatic vessel. The likelihood of the disease returning is affected by the aggressive biology of the melanoma cell and its ability to survive for long periods of time.
It has been noted that the relapse process is typical for young people from 30 to 50 years old, and the timing of progression is associated with gender. For example, damage to regional lymph nodes in women occurs in the first year after removal of melanoma, in men - in the second or third, distant metastases in a man are likely in the first 3 years after treatment, in a woman - after 3 years.
The thickness of the first tumor correlates with the rate of progression; with a thickness of more than 2 mm, 8–9 patients out of ten are likely to develop metastases in the lymph nodes. In clinical studies, a standard approach to the distance from the tumor to the incision line has been developed, depending on the thickness of the tumor node, so at least half a centimeter is retreated at a minimum height, with a nodule thickness of more than 2 mm, 2 centimeters are retreated from it.
As we recently found out, the probability of recurrence has little effect on the volume of the primary operation, but if the volume of excision is insufficient, when malignant cells are found in the edges of the removed tissue during histological examination, a repeat operation is performed no later than 8 weeks or radiation is carried out with preventive drug therapy.
Preventing the appearance of a new mole
Before surgery to remove a mole, it is recommended to undergo a histological examination, which will determine the nature of the neoplasm. This diagnostic method is considered the most accurate. After confirming the benignity of the nevus, you should choose the best clinic and doctor who has sufficient experience in this field. Next comes the selection of the removal method. There are many of them, so it is necessary to choose the safest method that guarantees complete removal of the tumor. To avoid unpleasant consequences after removing a mole, you must follow the recommendations that the doctor must give:
- Do not wet the area where the growth is removed for the first 7 days.
- Properly treat the damaged area of skin. Before handling, wash your hands thoroughly to avoid infection.
- After 1 week, a dry crust will appear on the wound, which under no circumstances should be removed. The dead skin will fall off on its own over time.
- If the operation is performed in the summer, you should avoid prolonged exposure to the sun, do not sunbathe, and do not visit the solarium. If you cannot avoid direct sunlight, the wound should be covered with clothing, and a bactericidal patch can be glued on top. Exposure to ultraviolet radiation can cause the appearance of pigment spots in areas of skin damage.
Compliance with careful care of the affected area after removal of a mole is the key to successful recovery and prevention of recurrence of the tumor. If scars begin to appear on the skin, it is necessary to use ointments and creams, the therapeutic effect of which will help hide such cosmetic defects. Properly done independent and medical work will lead to a good result.
Locations
Two thirds of relapses are metastases, one third are nodular formations in the area of the first operation. The location of the maternal tumor affects the fate of the patient:
- every third person operated on for melanoma of the scalp and neck develops tumors in the scar, and in women the problem occurs in the first year after treatment;
- transit metastases have the largest percentage in the group of melanomas of the extremity; this type of progression in women develops five years after excision, and in the male population - in the second and third years after surgery;
- with the initial lesion of the skin of the legs most often, in seven out of ten secondary tumors are found in the lymph nodes, in women in the next year, in men a little later;
- The primary process on the trunk in every fourth person is complicated by distant metastases.
Signs and symptoms of melanoma
Signs of recurrent formation in the skin and soft tissues do not differ from those of a primary tumor; the same diagnostic algorithm is applicable to them: asymmetry and uneven coloring, uneven edges and instability of the condition. The sizes are very variable - from tiny to gigantic, “the size of a baby’s head.”
Symptoms of metastases depend on the location, so if the lungs are affected there may be a cough with shortness of breath, if metastases to the brain - blurred vision, headaches, vomiting, convulsions.
Regional metastasis is manifested by an increase in the package of lymph nodes, followed by tumor growth into soft tissues and blocking of nearby passing vessels, which is complicated by swelling of the limb.
Clinical studies have proven that detecting disease progression before symptoms appear significantly improves life prospects. The course of the disease is always individual, so observation after treatment should be based on the biological characteristics of the malignant tumor. The European Clinic does everything for early detection and prevention of health problems.
Relapse groups
In 1985, the domestic oncologist Anisimov proposed, for the convenience of describing the clinical picture, to divide recurrent tumors into six groups:
- The first - round and few formations, often outside the scar and mainly subcutaneously - in the fatty tissue, often fall under the criteria of “transit” metastasis according to Wagner.
- The second is multiple irregular cutaneous and subcutaneous infiltration accompanying vessels and nerves; it is assumed that the external picture of relapse is formed by tumor cells that have taken root in small vessels.
- The third is nodules directly associated with the operation area that have grown from malignant cells remaining in the skin.
- The fourth is polycyclic multiple formations.
- The fifth is a lot of bulging nodules, often on a stalk, like morel mushrooms.
- The sixth is a combination of all five options.
Classification is rarely used in clinical practice, because the assessment of treatment results is based solely on the size of the nodes, and not on their appearance.
If there was no histology.
Calmly remember whether the doctor performed any additional research methods. Dermatoscopy? Scraping or puncture?
If yes, with a probability of about 95%, everything is fine and this is really a relapse of the nevus, and not melanoma. It requires nothing more than observation and, most likely, will not grow or change.
If there were no other examinations or histology, it seems to me advisable to excise the relapse with mandatory histological examination.
Yes, this is not easy or pleasant, but only such a step can confirm the absence or presence of melanoma.
If a mole, which was removed without histology, not only appears again, but has grown to its previous size, you need to go to an oncologist URGENTLY.
Frequency of occurrence
For any type and size of melanoma, the most common progression after surgery is metastases to other organs in almost 60% of patients.
The most dangerous period is the first three years after surgery, but in the first year, 60% are more likely to have metastases in regional lymph nodes. In stages 1 and 2, the incidence of lymph node involvement is low - every fifth person, and very rarely - less than 5% are affected by the postoperative scar.
Due to the development of relapses of the disease, only 60% of patients live longer than five years, but the disease can return after 15 years - in 7%, and after 25 years - in 10%. Every fifth person with an unimportant individual prognosis, however, does not experience a relapse in the next 5 years.
The nature of the tubercles formed
The tubercles that may appear at the site of excision of nevi, in most cases, represent an infiltrate that develops with severe trauma to tissue structures, poor hemostasis (blood clotting), or infection. They look like cellular structures that are permeated by lymphatic fluid or blood. The formation of this element has an inhibitory effect on healing or completely stops this process.
The formation of a non-inflammatory infiltrate occurs in the postoperative period. It is represented by tissue that is saturated with lymph or drugs, without signs of an inflammatory process. Typically, such seals disappear without outside intervention after some time: healing takes weeks, sometimes months. Special regenerating medications and physiotherapy help speed up resorption. If inflammation develops, contacting a doctor is a must.
We invite you to familiarize yourself with the most effective masks for treating blackheads of comedones at home
Diagnostics
The examination is similar to the diagnosis of the primary process. A special feature of diagnosing progression is strict adherence to a schedule of regular examinations, which makes it possible to identify the process at the very beginning and before the appearance of clinical symptoms.
In European countries, it is recommended to visit an oncologist every 2 months during the first year after surgery, quarterly in the second year, and then be monitored without reducing intensity, since most often relapses occur in the first three years.
Early diagnosis of melanoma relapse is an objective reality today. In each clinical case, the European Clinic uses an individual diagnostic search program, eliminating both the redundancy of the examination and its insufficiency.
Is it necessary to remove it again?
Diagnostic methods allow us to objectively study the condition of a person’s skin. Effective options are:
- examination in a specialized clinic;
- performing dermatoscopy;
- digital analysis of tumor growth (in dynamics);
- formation of a “map” of structures at a specific location;
- performing a skin biopsy.
Dermatoscopy is the process of examining the skin using a specialized apparatus. A physician can examine the internal structure of the growth and classify it. Afterwards, an effective treatment plan is selected. An equally informative diagnostic method is a puncture biopsy. The research mechanism involves manipulation of a special needle.
Signs of a mole healing after removal are:
- a dry dark crust remains on the operated area;
- the size of the keratinized structure is 1 mm;
- after a couple of weeks the growth will peel off from the skin;
- the formation of a small red pit, the depression does not exceed 1-2 mm;
- after 28 days, the bottom of the fossa gradually rises to the epithelial level;
- 90 days after the intervention, the inflammation disappears, and an invisible unevenness or scar remains from the mole.
If a light-colored liquid flows out from under the crust, this is a good sign, which means the treatment is going according to plan. To keep complications to a minimum, follow all doctor's instructions. The incisions are treated with high-quality antiseptics.
Oncologists and dermatologists agree that recurrence of nevus is only in rare cases dangerous to human health. The risk of melanoma formation increases markedly if the operation was performed without dermatoscopy. Taking a scraping or puncture will allow you to clearly determine the causes of the development of the pathology.
We suggest you familiarize yourself with a lump left after a boil: what to do with a lump under the skin
It is not recommended to remove tumors using cosmetic surgery. Unskilled impact on the structure leads to complications. It will be a shame when a person faces cancer due to negligence or inattention. It is better to perform procedures in specialized institutions. Before the mole removal process, a high-quality skin diagnosis should be performed. Otherwise, you increase the likelihood of additional complications.
There is nothing wrong with the appearance of moles on the body, but sometimes the reason for their occurrence is fraught with many mysteries. The first nevi appear in infancy, and the rest can be acquired throughout later life. Sometimes it happens that you have a mole removed, and it appears again, but why does this happen?
Treatment
Treatment of local recurrence in the scar, transit metastases and altered lymph nodes is similar to the tactics for the primary tumor - surgery is optimal, including plastic closure of a large tissue defect.
Adjuvant drug treatment after surgery is the norm; drugs that have not previously been used for prevention are used, although the choice is small: alpha-interferon and ipilimumab.
With metastases to other organs, the question of drug therapy arises, and in the first line they resort to immuno-oncological drugs in combination with targeted drugs in the presence of gene mutations.
The choice of drugs is large, therefore, in the absence of results or progression during second-line treatment, they resort to previously unused drugs. Chemotherapy for relapse of melanoma is used as a last resort, not because of pronounced adverse reactions, the problem is the low result. For superficial formations, radiation therapy is possible.
Why is relapse dangerous?
Relapse in melanoma is not only the appearance of a malignant formation in the scar, but also metastases. They most often affect the lymph nodes, lungs, skin, brain and liver. The possibility of removing a recurrent formation opens up prospects for a long life; if the operation is technically impossible, then the present and future will be occupied by drug therapy.
Survival for multiple organ metastases does not exceed six months; the results of drug therapy leave much to be desired, even with the use of innovative immuno-oncological drugs, which rarely promise more than two years of life.
Brown dot - what is it?
Sometimes, some time after the mole has been successfully removed and the skin has healed, a dot appears in the same place. Most likely, such a spot is a symptom of a relapse - the reappearance of a nevus. It may take 1-2 months from the moment of surgical removal to the visual appearance of a new mole, sometimes more.
When you carefully examine the brown spot that appears at the site of the removed mole, under a microscope you can see cells that are typical for all moles. They are capable of producing a brown pigment known as melanin. It is thanks to him that the nevus turns brown.
Forecast
Every year, melanoma is diagnosed in an average of 15 people out of every hundred thousand adults, approximately 3 patients die, and with a fairly stable mortality rate in the last quarter century, men began to die more often. Gender determines a lot in the prognosis of the disease, other things being equal, but young people experience the disease with less difficulty.
The probability of death with a late relapse is many times lower than with an early relapse. Early detection of progression promises better treatment results.
It is extremely difficult to predict the course of melanoma, because even a common process is not considered absolutely fatal; this malignant disease does not often live up to expectations. Don’t guess “to be or not to be”, contact specialists if you have problems, or better yet, before they appear - we will always help.
| Read more about dermatological research at the European Clinic | |
| Consultation with a dermatologist-oncologist | from 5100 rub. |
| Skin examination using the German FotoFinder device | 12100 rub. |
| Diagnosis of melanoma | from 5100 rub. |
Book a consultation 24 hours a day
+7+7+78
Bibliography
1. Semiletova Yu.V., Anisimov V.V., Vagner R.I. /Treatment of patients with primary skin melanoma. Current state of the problem // Siberian Journal of Oncology. 2010. No. 4. 2. Semiletova Yu.V., Anisimov V.V., Lemekhov V.G. et al./Risk factors for relapse after radical treatment of skin melanoma//Sibir.onko.zhur.; 2012. No. 2 (50) 3. Stroyakovsky D. L., Abramov M. E., Demidov L. V. et al. /Practical recommendations for drug treatment of skin melanoma // Malignant tumors: Practical recommendations RUSSCO #3s2, 2018 (volume 4. de Vries E., Bray FI, Coebergh JW, Parkin DM /Changing epidemiology of malignant cutaneous melanoma in Europe 1953–1997: rising trends in incidence and mortality but recent stabilizations in western Europe and decreases in Scandinavia// Int J Cancer 2003; 107. 5. MacKie RM, Bray C., Vestey J., et al./Melanoma incidence and mortality in Scotland 1979– 2003 // Br J Cancer 2007;96.
/Treatment of patients with primary skin melanoma. Current state of the problem // Siberian Journal of Oncology. 2010. No. 4. 2. Semiletova Yu.V., Anisimov V.V., Lemekhov V.G. et al./Risk factors for relapse after radical treatment of skin melanoma//Sibir.onko.zhur.; 2012. No. 2 (50) 3. Stroyakovsky D. L., Abramov M. E., Demidov L. V. et al. /Practical recommendations for drug treatment of skin melanoma // Malignant tumors: Practical recommendations RUSSCO #3s2, 2018 (volume 4. de Vries E., Bray FI, Coebergh JW, Parkin DM /Changing epidemiology of malignant cutaneous melanoma in Europe 1953–1997: rising trends in incidence and mortality but recent stabilizations in western Europe and decreases in Scandinavia// Int J Cancer 2003; 107. 5. MacKie RM, Bray C., Vestey J., et al./Melanoma incidence and mortality in Scotland 1979– 2003 // Br J Cancer 2007;96.