Skin melanoma is a rare tumor that is malignant in 5% of cases. Using the Clark classification of melanoma grade allows for an initial assessment and determination of tumor development. This classification determines the depth of germination into the skin and deep tissues. After tissue histology, according to Clark's classification, radiation treatment or chemotherapy is prescribed. Cutaneous melanoma is a malignant tumor that accounts for about 1.4% of all tumors in women and 0.8% in men.
The Clark method for determining melanoma allows you to study the degree of danger of skin tumors.
Severity classification
There are several possible types of classification of melanoma severity, which are actively used by doctors. Among them are:
- Microstages according to Clarks.
- Breslow stages.
- TNM classification system.
- Stages according to the TNM and AJCC systems.
When determining the severity of a tumor formation, they talk about staging melanoma. Diagnosis is carried out by a specialist dermatologist-oncologist based on the following studies:
- Medical examination.
- Applications of a dermatoscope.
- Histological examination.
- Biochemical blood tests.
- Other diagnostic methods, in particular ultrasound, CT and MRI diagnostics, as well as radiography.
By correctly identifying the severity of the disease, doctors can select truly effective methods of therapy to get rid of melanoma in each specific case.
According to Clark
The Clark method of classifying tumor severity has been used by physicians for more than 50 years and takes into account the degree of tumor invasion into skin structures. There are 5 levels of melanoma:
- Level 1. In this situation, all cancer cells remain within the epidermal layer and do not affect the basement membrane. This is how melanoma in situ manifests itself (pre-invasive cancer or stage 0 cancer).
- Level 2. The layer of basement membrane that separates the epidermis from the dermis suffers from the aggression of tumor cells that begin to invade the upper, papillary layers of the dermis.
- Level 3. In this case, the papillary layer is filled with atypical melanocytes, but they have not yet descended into the area of the reticular layer.
- Level 4. Melanoma breaks into the reticular layer.
- Level 5. With this development of the tumor, its cells can already be detected in the area of subcutaneous fatty tissue.
Today, diagnosis using Clark levels can only be used in situations where doctors, for some reason, are unable to determine the intensity of tumor cell division.
Minuses
The Clarks diagnosis does not take into account several very important criteria that allow us to draw conclusions about the characteristics of cancer, in particular:
- Its thickness (the determination of tumor thickness is the basis for the Breslow classification of this cancer).
- Presence of microscopic ulcerations. This allows us to judge the intactness (undamaged) of the epidermis, which covers a significant part of the tumor formation.
- The rate of mitosis is the division of pathogenic cancer cells.
According to Breslow
The modern approach to the diagnosis and correction of melanoma necessarily takes into account the thickness of the tumor. After all, the more subtle the melanoma, the greater the patient’s chances of recovery. Therefore, Breslow thickness is considered as a fairly important factor in predicting the progression of the disease. Depending on their thickness, tumors have the following levels of complexity:
- The thickness of the dermal component is no more than 0.75 mm.
- Thickness from 0.75 to 1.5 mm.
- Thickness from 1.51 to 3 mm.
- Thickness from 3.1 to 4 mm.
- Thickness over 4.1 mm.
It is worth noting that the presence of microscopic ulcerations increases the severity of cancerous tumors. The presence of such a symptom can move the formation to a much later stage, even if it is quite small in size.
TNM classification
The TNM system is considered today the main method for classifying cancer, which is understandable to specialists from all over the world. It allows you to accurately and in great detail describe the morphological changes in tumor formation, taking into account the stage of tumor growth. TNM includes the following characteristics:
- “T” - tumor - the tumor itself (in particular, its thickness, existing ulcerations).
- “N” - nodus - nodes (degree of damage to nearby lymph nodes).
- “M” - metastasis - metastases (distant).
The TNM stage can be determined only after complete removal of the tumor and comprehensive diagnostics.
Criteria for evaluation
To identify the exact stage and characteristics of tumors according to the TNM system, the following criteria are used for category T:
For category N:
For category M:
When using the TNM classification, the final diagnosis sheet indicates three criteria at once, which allows doctors to accurately determine the strategy for further therapy.
TNM and AJCC
This method of classifying melanoma makes it possible to determine the exact stage of the disease depending on TNM criteria:
A refined classification allows you to make the diagnosis as accurate and informative as possible. It is this that is taken into account when choosing a protocol for treating the disease, which is followed in various countries, and the effectiveness of which has been confirmed for many years.
Features of the Clark flow
The prognosis for stages 1 and 2 can be according to Clark:
- At the first stage of invasion, the neoplasm is located within the dermis.
- At the second level, according to Clark, the tumor spreads into the papillary layer of the skin.
- At the third level, the neoplasm reaches the border between the reticular and papillary layers of the skin.
- At the fourth stage, according to Clark, germination occurs in the reticular layer of the skin.
- In the fifth stage, the tumor spreads into the tissue under the skin.
At the very last stage of the disease, the tumor penetrates the skin
Treatment
Melanoma therapy can only be carried out in specialized oncology clinics. The early stages of the disease are quite treatable, since during their development only the skin is affected, and the tumor itself does not reach the deep layers, and also does not affect the lymph nodes and other organs. The treatment regimen is selected according to a standard protocol, depending on the characteristics of the identified tumor.
Initial or 0
While the tumor cells are still within the epidermis, melanoma is easiest to treat - it simply needs to be removed by wide excision, involving the surrounding healthy skin. Removal is carried out using a scalpel, since this method is considered especially effective for cancer. All removed material is examined and, if necessary, treatment is supplemented. In particular, if cancer cells are detected at the edges of the excised fragment, radiation therapy or re-resection of the lesion may be required. Local application of a cream with imiquimod, which is an immunomodulator and modifier of the immune response, is often prescribed.
Stage 1
At the first stage of melanoma, a wider excision of the lesion is required along with the capture of a fairly large amount of healthy skin (up to two centimeters from the edge of the tumor formation).
If necessary, the doctor may insist on performing a biopsy of a nearby lymph node (if there is a suspicion that it may be involved in the tumor process), and if cancer cells are detected in it, removal of all nearby lymph nodes is required. Additionally, therapy with immunomodulators is carried out.
2 stages
In the second stage of melanoma, the prognosis for the patient is still quite favorable, since the tumor has not yet affected the lymph nodes, therefore, treatment also involves wide excision. Doctors remove the tumor and healthy skin around it, and also necessarily examine the “sentinel” lymph node to detect cancer cells. If necessary, all nearby lymph nodes are removed. Patients with stage 2 melanoma are indicated for additional treatment aimed at preventing relapse of the disease.
3 stages
When the tumor reaches the lymph nodes, therapy should be more extensive:
- Mandatory excision of the melanoma itself is carried out along with part of the healthy skin.
- Lymph nodes are removed.
- Interferon therapy may be required to prevent relapse.
- It may be necessary to administer radiation therapy to the areas of the excised lymph nodes.
In addition, treatment may include the use of special vaccines, chemotherapy and targeted therapy. Biochemotherapy is also sometimes performed, which combines chemotherapy and immunotherapy.
Sometimes patients decide to participate in clinical trials of various latest developments by world doctors. This departure from the standard protocol is not a guarantee of success, but sometimes it can achieve positive results.
4 stages
This is the most difficult stage of melanoma to treat and requires excision:
- Tumors on the skin.
- Affected lymph nodes.
- Metastases in internal organs (if possible).
The success of surgical treatment is determined by the number of affected areas, their location, and the symptoms present. If metastases are detected that cannot be excised, the following is performed:
- Radiation therapy.
- Targeted therapy.
- Chemotherapy.
- Immunotherapy.
Unfortunately, today stage 4 melanoma is considered practically incurable. However, targeted treatment makes it possible to prolong the life of patients and make it as comfortable as possible.
Stages
At the third stage of melanoma, experts distinguish three phases of the development of the disease - A, B and C. So, using this information, we can distinguish the following stages of development of stage 3 melanoma:
- 3A
(categories T1a – T4a, N1a or N2a, M0). The nearest lymph nodes are already affected, but not yet enlarged, distant metastases are not observed, and the thickness of the tumor is not precisely known. - 3B
(categories T1a – T4a, N1b or N2b, M0). The affected lymph nodes are already enlarged in size. However, no distant metastases are observed, and the thickness of the tumor is also not revealed. - 3B
(categories T1a – T4a, N1c, M0). The thickness of the melanoma was not revealed. But it has already spread to the nearest areas of the skin and into the lymphatic channels, but the lymph nodes themselves are not carriers of metastases. No further spread of the tumor is observed. - 3C
(any categories T, N3, M0). The thickness of melanoma may or may not be detected. It has already spread to several nearby lymph channels and crowded lymph nodes. However, distant spread of the tumor is not observed.
Life expectancy forecast
When doctors talk about the prognosis for life with melanoma, they emphasize that successful recovery directly depends on early diagnosis and timely treatment. Fortunately, skin cancer is much easier to detect than other types of cancer. In addition, surgical treatment methods and drugs for antitumor therapy are being improved every year. However, it is worth considering that melanoma exhibits the ability to grow very quickly, so if any suspicious changes appear on the skin, you should not delay contacting a doctor.
A few words about the forecast
You may be disappointed by the survivability information above. However, when considering this issue, it should be kept in mind that behind the statistics there are numbers, not a specific patient. This is an average, so it is difficult to predict how you will respond to treatment. In addition, science does not stand still; approaches to treatment are constantly being improved. The effectiveness of many of them is currently being tested in clinical studies. Statistics always lag behind the real state of affairs by several years, and their indicators do not reflect today's results of treatment effectiveness.
How long do they live?
Life expectancy for melanoma depends on the stage of the disease. To assess the survival prognosis, periods of 5 and 10 years are taken:
If you carefully examine the table, it becomes clear that the prognosis for patients with stage 3 melanoma is sometimes better than for patients with a stage 2 tumor. We can also conclude that even stage 4 is not a 100% death sentence, and with such a diagnosis there is a chance of living for more than 10 years, especially if the metastases spread throughout the skin and lymphatic system, but do not affect other organs.
What affects survival?
The prognosis for patients with melanoma depends primarily on the stage of the melanoma, but is also affected by:
- Localization of the tumor. It has been noted that life expectancy is higher in those patients in whom melanoma forms on the forearms or legs, and shorter in those in whom it is found on the scalp, hands, feet and mucous membranes.
- Patient's gender. Statistically, women have a better prognosis than the stronger sex. Perhaps this is explained by the girls’ greater attention to their own health.
- Age. For the elderly, the prognosis in general is not very favorable, which is largely explained by the general “wear and tear” of the body.
- Color of the skin. Melanoma is rarely diagnosed in people with black skin, but if they develop this disease, the prognosis is very unfavorable.
- The work of immunity. If the body's defenses are weakened, the prognosis for recovery worsens.
Even if the prognosis for melanoma is not very favorable, in no case should you refuse treatment. The development of cancer and the disease’s response to therapy is highly individual, and sometimes it is possible to achieve success and recovery even in the last stages of the disease.
Types of melanoma.
According to the Australian classification of melanomas, these tumor diseases of the skin are usually divided into four main types: • superficially spreading; • nodular, or nodular; • lentigo melanoma; • acral-lentiginous;
According to WHO, these four types account for about 85% of all diseases of this pathology. Let's take a closer look at each of them.
Superficial spreading melanoma
This type of melanoma is the most common and, according to various authors, accounts for 65 to 80 percent of all cases of primary melanoma. People of both sexes of the Caucasian race between the ages of 30 and 50 are most susceptible to it. The appearance of this pathology is associated primarily with prolonged exposure to direct solar radiation. In the stronger sex, this disorder is more common on the head, neck and torso, and in women it affects the skin of the lower extremities.
There are two phases in the development of this type of melanoma:
- Radial growth stage. During this phase, melanoma appears as a brown patch on the skin with pinkish or dark spots. The spot may protrude above the surface of the skin and has clear, irregularly shaped edges surrounded by an area of redness. Over time, this spot grows laterally and, thickening, becomes a dark, shiny plaque.
- Vertical growth stage. At this stage, a node forms in the flat tumor, which can ulcerate and bleed. In addition, malignant cells begin to penetrate deeper layers of the skin and can lead to the appearance of metastases in neighboring organs and tissues.
More about superficial spreading melanoma
Nodular or nodular melanoma
This type of melanoma is more common in males over the age of 50. It can occur in any part of the body and accounts for about 15% of all cases of primary melanoma. Often its development begins at the base of a nevus, or mole. Such a mole suddenly changes its color towards darkening and increases in size both upward and to the sides.
Nodular melanoma practically does not have a radial growth stage - with it, the formation of a round-shaped tumor node with clear edges immediately begins. Because of this, this type of disease is characterized by rapid development with intensive formation of metastases and a poor prognosis.
All about nodular (nodular) melanoma
Lentigo melanoma
This type of disease accounts for about 10% of all cases of skin melanoma. The most common occurrence of lentigo melanoma is in people who work outdoors for a long time and are constantly exposed to direct sunlight. Most often, this pathology develops on the scalp, neck and hands - that is, on those parts of the body that are not covered by clothing. In addition, it may appear on the lower extremities or on the back. Women are twice as likely to suffer from lentigo melanoma than men. In addition, this form of malignant tumor occurs mainly in old age.
- The radial growth stage of tape melanoma is quite long and sometimes lasts up to 20 years. In this phase, it looks like a brown spot with irregular outlines, reminiscent of a geographical map, and a clear edge. There are black inclusions on the surface of the spot, and its size can be 3-20 cm.
- The vertical growth stage also lasts several years. As it progresses, the spot enlarges and rises above the surface of the skin. In addition, the relief of the neoplasm also changes - a node forms on it, which sometimes causes an itching sensation. Often such a node loses color, may bleed, and crusts periodically form on it.
Lentigo melanoma rarely forms metastases compared to other types of skin tumors. This is due to its predominantly favorable course and prognosis.
Read more about lentigo melanoma
Acral lentiginous melanoma
This is the rarest type of melanoma - it accounts for less than 10% of all cases of the disease. Acral lentiginous melanoma most often develops on the thick skin of the hands or feet, as well as in the nail beds of the fingers. No patterns in the frequency of occurrence of this form among different races, sexes or ages were identified.
The clinical manifestations of this type of melanoma are very similar to the superficial form. There will be differences only when melanoma develops on the nail bed. At first, the swelling looks like a brown line on the nail plate. Changes detectable by touch appear only in the vertical growth phase. The neoplasm increases in size and raises the nail plate, which is accompanied by pain, splitting and degenerative phenomena in the nail. This form of melanoma has a rapid course and a high risk of metastases, and, therefore, a poor prognosis.
More about acral-lentiginous melanoma
VII
Last days
Absolutely unfavorable prognoses from doctors force patients with skin cancer in the final stages to think about their not very rosy future. But experienced world doctors assure that such thoughts only worsen the condition and bring death closer. With advanced cancer, patients need palliative care, which includes three main approaches:
- Relief of pain and symptomatic treatment.
- Psychological support.
- Social support.
Today, palliative medicine in our country is still in the early stages of development. Nevertheless, you can get the necessary support and assistance even in not very large cities. Every year quite a lot of paid hospices and palliative care departments are opened, which become an excellent alternative to public clinics.
Life after removal
Even after successful removal of melanoma, the disease can recur. The patient may also develop new tumors. Therefore, to maintain your health in the future, you must definitely consult with doctors and develop an individual monitoring plan:
- Approximate schedule for performing examinations and various tests.
- Possible schedule for additional studies that may be necessary.
- List of normal side effects of therapy. Such a list will make it possible to understand which reactions are abnormal and require immediate medical attention.
- A list of health characteristics that require particularly close monitoring.
In addition, the doctor must inform the patient about the recommended diet, physical activity regimen and existing restrictions. If you have any questions, you should seek answers from doctors.
Monitoring your condition after surgery
After a successful discharge from the hospital, a patient with operated melanoma will need to be regularly checked by a doctor and monitor his condition independently. Postoperative follow-up should include:
- Systematic examination of the skin and lymph nodes.
- Carrying out control instrumental studies, for example, radiography, PET, computed tomography, etc. Such clinical observations are usually not indicated for patients with stage 1 of the disease.
- Conducting local irradiation of the area of the tumor defect, as well as the use of special immune drugs. Such therapy helps prevent relapse of the disease, but is not carried out in all cases.
The regularity of follow-up examinations directly depends on the stage of the detected tumor process:
- If the tumor was at an early stage, you need to visit a doctor once every six months to a year for several years. The absence of alarming symptoms allows you to extend the intervals between visits to the clinic over time. The presence of a significant number of moles requires more frequent observations.
- If thicker or more widespread tumors were removed, it is necessary to be observed by a doctor at intervals of 3-6 months. for several years.
Those patients who survived the discovery of melanoma at stages 3 and 4 must definitely visit a doctor in accordance with an individually established schedule. The specialist can adjust the prescribed treatment and note the dynamics of the process.
DIAGNOSIS OF MELANOMA
Diagnosis of melanoma can be divided into “BEFORE” and “AFTER”
1. BEFORE , or otherwise it is called “ prevention of melanoma ”. Everything is simple here. Anyone should undergo regular skin examinations. Especially if he has a large number of moles. Especially if he likes to visit hot countries and sunbathe there until he turns blue. Especially if he has large moles.
The examination must be carried out by a doctor. The principle of ABSD, which is shown on TV, does not always work in determining melanoma. You will not be able to distinguish a normal mole from a melanoma on your own.
The examination should be carried out not according to the “show me and I’ll look” principle, but according to the “undress and lie down” principle. The examination is carried out starting from the head and ending with the heels. If the dermatologist is not going to do this, then change the doctor.
The examination is carried out using a dermatoscope! This is a must.
Before visiting a dermatologist, examine your “intimate areas” yourself, using a mirror, or ask your spouse. Moles found in these places must be shown to a doctor!
If you think that a person with the profession of DOCTOR (and especially a dermatologist, surgeon, oncologist) is embarrassed by what is in your underpants, then you are deeply mistaken. If the doctor himself has problems with this matter, then just change him - such specialists are walking through the woods.
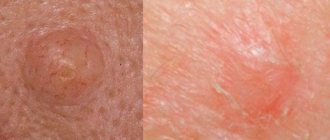
The fact is that the diagnoses of “ melanoma of the penis ” or “ melanoma of the labia ” have not yet been canceled. Here is an example of a discovered and removed dysplastic nevus located between the patient’s buttocks: Treatment of melanoma in Israel. The review and all this can be called funny and stupid, but only until you hear one of the above diagnoses.
And I also want to note that the location of your tan has NO correlation AT ALL with the location of the possible appearance of melanoma .
And of course, the most advanced control method is to compile a map of moles and update it annually. Something like this:
Diagnosis of skin cancer at the Melanoma Unit clinic in Israel
You can read more here: Digital dermatoscopy in Israel
2. After.
So, you had your melanoma removed.
The first thing you should see is the result of the histological examination, which should contain the following parameters:
Tumor thickness according to Breslow (IMPORTANT! For thin melanomas, accuracy to hundredths of a millimeter is VERY important) Level of invasion according to Clark (When the tumor thickness is about 1 mm, this parameter loses its value and is replaced by the mitotic index) Presence/absence of ulceration - the presence worsens the prognosis Mitotic index - presence worsens prognosis
Example: Melanoma, Breslow thickness less than 1 mm - this is a very approximate result, which indicates the low quality of the laboratory and the equally low qualifications of the oncologist who is satisfied with this result.
I would also like to note that errors in histological studies are a common and regular phenomenon, therefore, histology needs to be reviewed and the final authority (in my experience) is Israeli pathologists.
If the pathologist cannot accurately determine whether it is melanoma or not, then another test called immunohistochemistry is used. It should be noted here that the S100 tumor marker is used specifically for painting “material”, but not for diagnosing melanoma by blood.
Further:
a) If the tumor thickness is <0.5 mm and the mitotic index is 0 , be happy, you don’t need to do ANYTHING . Yes, you can go for preventive examinations to the doctor once every three to six months, but you must understand that you are really lucky .
b) But everything that is thicker and more aggressive ( has a mitotic index >0 ) requires closer attention.
You need to understand that by “diagnosing melanoma” we mean searching for the presence/absence of metastases , because the melanoma itself has already been removed and we are no longer particularly interested in it, as well as identifying new tumors on the skin (but everything is simple here - see point 1)
To diagnose melanoma the following are used:
Ultrasound is the most common and simple/available/cheap method. An intelligent ultrasound specialist is important here, because the majority of “specialists” are unlikely to be able to find “something” less than 4-5 mm in size, while a professional has a chance to lower the millimeter bar to 3x.
Ordinary X-ray of the lungs (or fluorography, I always confuse it)
Computed tomography (CT) is more serious. Only it needs to be done on the entire body, and not on a “separate area”. It can be performed with or without a contrast agent (preferably C).
Magnetic resonance imaging (MRI) - used only to study the brain. The same can be done with or without contrast.
Well, the most advanced method for detecting metastases is positron emission tomography combined with computed tomography (PET CT). Here is an example: PET CT scan at the Assuta clinic
Anyone who is found to have enlarged and suspicious lymph nodes may require an “ultrasound-guided fine-needle biopsy .
Sentinel lymph node biopsy is the most important procedure that allows you to determine the presence of micro metastases in the sentinel lymph nodes, and helps stop the spread of melanoma at the very initial stage (see the corresponding section above)
Example : photo of one melanoma cell that was discovered in a lymph node during a sentinel biopsy
The choice of diagnostic methods (one-time and regular) is made by a doctor whom you trust.
XI
Is it possible to sunbathe?
Surprisingly, the question of the possibility of tanning is of great concern to patients who have undergone melanoma removal. In fact, exposure to ultraviolet rays with a history of such a diagnosis becomes one of the risk factors and can lead to relapse of the disease and the appearance of new tumors. Therefore, doctors still recommend avoiding sunbathing or visiting a solarium.
Prevention
In order to prevent the formation of a malignant process on the skin, it is necessary to adhere to certain rules:
- Do not visit the solarium.
- Limit sun exposure. While sunbathing, cover potentially dangerous moles.
- Use sunscreen for your skin with a filter of at least 15.
- Periodically inspect the entire body for suspicious formations.
- Borderline and dysplastic nevi are best removed.
- If you have any suspicions, consult a doctor.
Relapse prognosis
Recurrence is said to occur when the tumor reappears after successful removal. In this case, a new formation may appear in the same place where the maternal melanoma is or near it, as well as in distant parts of the body (local relapse is more common). Relapse can occur even 10 years after a successful recovery, and the risk of its development increases if:
- Significant thickness of the tumor.
- The presence of ulcerations in the primary tumor.
- Formation of satellite metastases surrounding the primary tumor.
- High rate of tumor cell division.
The likelihood of relapse can be reduced by limiting exposure to ultraviolet radiation, regular monitoring by a doctor and a healthy lifestyle. In particular, moderate physical activity, a healthy and nutritious diet, normalization of body weight and giving up bad habits play an important role.